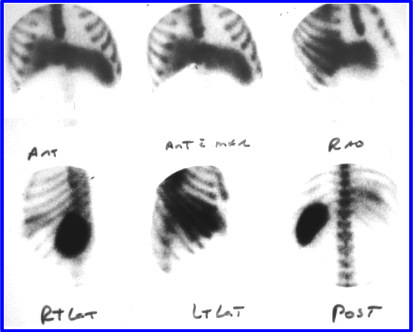
Six views are taken and normal radiopharmaceutical distribution is seen. Comments: Spleen and liver are of normal size; normal radiopharmaceutical distribution; and no bone marrow uptake.
- Metastatic liver disease (SOL)
- Cancer that spreads to the liver
- This may contain a single, but usually multiple - cold spots (I call it the swiss cheese effect)
- Towards end-stage this disease may mimic HD especially when there is extensive liver damage
- Typical types of cancer than metastasize to the liver include: breast, GI, lung, GU, pancreas, cervical, and ureter
- Leukemia and lymphoma involvement usually show diffused involvement
- Hepatomegaly is present in 50% of cases
- Improved detection is noted with SPECT with the resolution being: 1.5 to 2.0 cm
- Consider SPECT imaging when looking for disease deep inside the right lobe
- In SOL, initial hepatobiliary images and SC images will look similar because the cells that pick these agents both share the same space
- Another example of metastatic disease
- Hepatoma (SOL)
- Primary tumor of liver that is uncommon in the US
- Approximately 2/3 of patients with a hepatoma have cirrhotic livers
- Tumor grows very slow
- May be difficult to differentiate from metastatic disease, however, hepatoma is usually a large mass growing in the liver as compared to small multiple masses seen in mets
- Patients that have undergone androgen therapy (removal of testicles to retard the growth of prostate cancer) have a higher incidence of hepatoma
- Hepatomas often invade portal and hepatic veins producing portal hypertension
- Here is an example of a Hepatoma (hepatocellular carcinoma) with the administration of a hepatobiliary agent. Images were taken 1 hour and 24 hours post dose. This SOL would have a similar appearance if sulfur colloid was administered
- Differentiation from hepatoma and pseudotumor (SOL)
- Hepatoma is vascular and may be seen in the arterial phase of a dynamic blood flow procedure, while pseudotumor is not
- Hepatoma is 67Ga avid, while pseudotumor is not
- Pseudotumors are fatty deposits in the liver that may also occur with a cirrhotic liver
- Abscesses are classified into two major (SOL) categories
- Intrahepatic abscess
- Hepatomegaly with one or more defects
- Clinical findings - fever over 101 oF, liver tenderness, RUQ pain, weight loss, anemia, leukocytosis, and elevated alkaline phosphatase
- Amoebic abscesses mostly occur in men, with only one defect, and is usually in the right lobe
- Pyogenic abscess are often multiple, located in either lobe, and show no preference between the sexes
- 67Ga may be used to distinguish between amoebic and pyogenic, where a bacterial infection would be gallium-avid
- Subphrenic abscess
- Abscess between the liver and the lung (diaphragm)
- Symptoms include: fever, leukocytosis, and URQ pain with a history of abdominal surgery, perforated ulcer, or appendicitis
- Use a liver/lung scan to determine if there is an area lacking uptake between both organs
- Radiation Injury
- Excessive radiation can destroy parts of the liver
- Threshold dose is 3000 rads in 30 days
- Recovery has been noted if the dose does not exceed 5000 rads
- RECs are more radiosensitive than hepatocytes
- Extrahepatic masses (SOL)
- Causes compression or displacement of the liver
- Cysts or tumors located in the kidney, adrenal, spleen, pancreas, mesenchymal tumors; or enlargement of the gallbladder, kidneys, spleen or skeletal deformity
- Cysts located in the liver (SOL)
- Shows up as single or multiple cold spots
- Polycystic disease usually occurs with a long history of liver enlargement with upper abdominal discomfort
- From the above example, what other diseases imaged with sulfur colloid might look similar to this?
- Hepatic adenoma and focal nodular hyperplasia (SOL)1
- Associated with oral contraceptives
- Have a tendency to hemorrhage
- Adenomas are mostly associated with oral contraceptives, are usually avascular, rarely multiple, likely to hemorrhage and become necrotic, and usually do not pick up colloid
- Focal nodular hyperplasia is sometimes associated with oral contraceptives; is always vascular, often multiple, rarely hemorrhage or become necrotic, and may pick up colloid (its liver tissue)
- Another example of FNH
- Cavernous hemangioma (SOL)
- Benign tumor that engulfs RBCs is usually located deep in the right lobe
- When imaged with sulfur colloid the lesion appears cold
- However, if labeled RBCs are injected, over time, the lesion will becoming increasingly hot as it engulfs red cell - link to lecture on this topic
- Infarct (SOL)
- Very rare
- Usually shows up as a cold spot
- Area becomes necrotic
- Hemorrhage
- Usually from trauma
- SPECT or multiple planar views are required to define the area that lacks activity
- Trauma often effects the spleen. Blunt trauma received by the abdomen may cause a tear in the diaphragm and spleen tissue can be implanted in the thoracic activity. This results in an accessory spleen. For more information go to the Spleen Lecture
- Always acquire an anterior view that includes the chest to look for an accessory spleen
- Superior Vena Cava Obstruction
- Increased pressure in this vein causes a "slowdown" in the venous system. The end result is increased colloid uptake at the portal hepatitis
- While colloid particles show an increase uptake at the porta hepatis (far left) the second imagine (center) shows reduced blood flow to the same area. Labeled RBC were adminsitered which does not show an accumulation of blood
- Hepatitis and cirrhosis (HD)
- Both diseases look similar
- Note how increased damage to liver affects the liver, spleen, and bone marrow uptake (see above)
- Cirrhosis (HD)
- Mild: Minimal decrease uptake in liver and minimal increase uptake in spleen
- Moderate: Hepato/splenomegaly, atrophy of left lobe, patchy colloid uptake due to edema
- Advanced: Little or no uptake in the liver, splenomegaly, and bone marrow uptake
- Other unusual cases
 1
1

http://slideplayer.com/slide/10962683/

 2
2
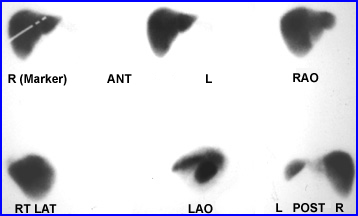
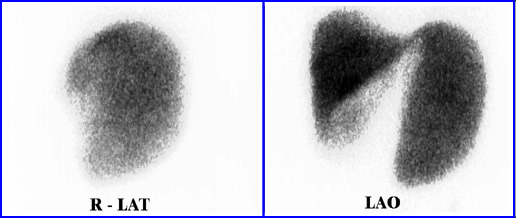
The next case is an example of space-occupying lesion(s). The main lesion is located in the upper right lobe of the liver and can be identified in every view that is taken. This photopenic area lacks activity because there are no Kupffer cells within the lesion; therefore, it lacks uptake of the radiopharmaceutical.
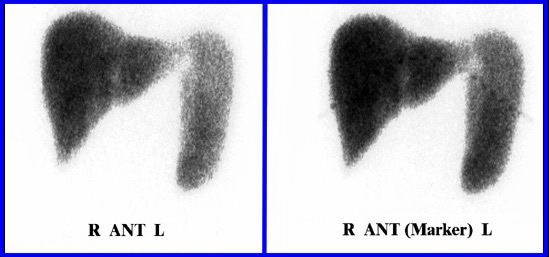
Here is an example of hepatomegaly and splenomegaly. This patient has an early stage of hepatocellular disease. The result is an increased size of the liver and spleen.


Fifteen minutes post injection the following image is taken of the liver and spleen. What is wrong with this picture?

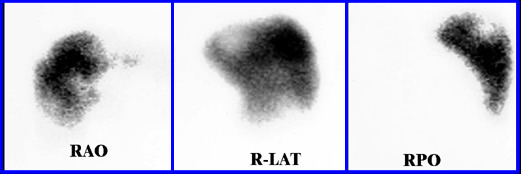
CT scan shows a large vascular tumor in the right lobe of the liver and is contrast avid. In image to the right shows normal colloid uptake in the right lobe. What would cause this abnormality?

The above three images are taken and discussed below
- Image A shows a CT slice with two major lesions. They are both avid with contrast
- Image B is the same patient, however, the patient has been injected with sulfur colloid
- Image C this same transverse slice shows complete filling in of the right lobe and some filling in in the left lobe
- What type of disease would cause this?
Return to the Beginning of the Document
Return to the Table of Content
10/18
References
1.a Nuclear Medicine Imaging by FA Mettler, et al. Chapter on Liver-Spleen Imaging - Hepatoma or hepatocellular carcinoma
1.b Focal lesions in the liver, liquid/solid, comment, Liver/Spleen Scintigraphy
- http://medcosmos.com/gastro/case31/c31g05.htm
2 and3) INTECH Chapter Three Clinical Applications of Nuclear Medicine and You Tube
4. Technetium-99M Sulfur Colloid Liver and Spleen Imaging - This link shows many difference types of liver disease when imaging with Sulfur Colloid
5. Nuclear Medicine Resources @ http://www.nucmedreview.com/cases/gi/gi.html
6. Mediscape - http://emedicine.medscape.com/article/368377-overview
7. The New England Journal of Medicine 2000; 342:791 http://www.nejm.org/doi/full/10.1056/NEJM200003163421106
8. Focal Lesion in the Liver: Solid.Liquid Comments, Liver/spleen scintigraphy, http://medcosmos.com/gastro/case31/c31g05.htm