- Two pair of endocrine glands that lie post to the thyroid, near the lateral aspect of each lobe
- Two superior and two inferior
- Average weight = 35 to 50 mg
- Enlargement (disease) of the parathyroid glands maybe do to
- Tumor
- Hyperplasia
 |
- Parathyroid Hormone (PTH) is synthesized and excreted by the parathyroid gland
- PTH levels regulate calcium and phosphorus levels within the body. As PTH increases this causes increase in osteocytes activity results in increased bone turnover resulting in increased serum calcium levels
- The opposite also occurs in that as levels of PTH decreased so does bone turnover resulting in lower levels of calcium
- The process of PTH secretion and calcium production is similar to thyroid's negative biofeedback loop
- Key - Ca+ is released into the blood stream from osteocytes activity caused by PTH production
- In addition, decreased levels of Ca+ results in increased levels of phosphates, sodium, and potassium
- Indirectly effects vitamin D in that vitamin D increases intestinal absorption of Ca+
- Primary Hyperparathyroidism is the result of increased levels of PTH production usually caused by caused by tumor or hyperplasia
- This increased PTH production causes hypercalcemia causing
- Nervous system depression
- Muscle weakness
- CaPO4 precipitates into the alveoli, arterial walls, gastric mucosa and renal tubules
- Death can results from renal failure
- Treatment is the surgical resection the tumor or resection of hyperplastic gland
- NMT is the only diagnostic procedure that can adequately examine this disease

- 201Tl is picked up by the parathyroid and the thyroid glands - mechanism for uptake is unknown
- 99mTcO4- is picked up by the thyroid only
- A subtraction technique can be used to determine if there is/are any tumor or hyperplastic tissue
- Following the subtraction method, any activity remaining is considered positive for tumor or hyperplasia
- This method is no longer used, but is very effective in finding disease
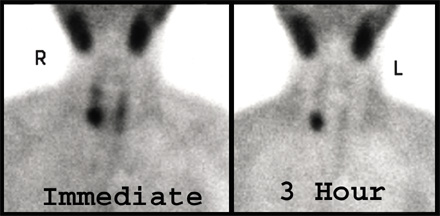
- 99mTcsestamibi
- Is the preferred method for finding disease of the parathyroid
- While the exact method of uptake is unknown an initial injection of the this agent will result in uptake of the parathyroid and thyroid gland
- Over time sestamibi washes out of the thyroid gland and remains in the parathyroid and more importantly tumor or hyperplastic tissue can be identified
- Any activity remaining after 3 hours post injection is either hyperplasia or tumor (usually an adenoma)
- Hyperparathyroidism
- Occurs in 1 out of 700 people
- 70% female
- Average age is 56
- Rare in children
- "Prolonged tracer retention within the parathyroid adenoma is felt by some to be related to the presence of mitochondria rich oxyphil cells within the lesion"1
Dual Phase Time Dependent Parathyroid Imaging
- Window setting 140 keV at 20%
- Preset time to 600 seconds
- Matrix size: 128 x 128
- Magnification at 1.5 if using high resolution collimator
- Collimator: High resolution or pinhole
- SPECT can be done on immediate and/or delays. The reason for this is to better localize the tumor
- 99mTcO4- can be administered after the delay images are taken. Rational - If there is an area of questionable uptake, it should be residual MIBI. Injecting technetium will differentiate the tissue from adenoma vs. thyroid