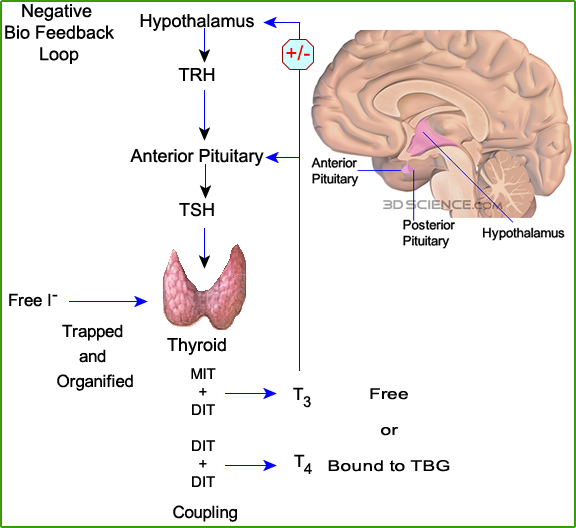
Physiology of the thyroid and the production of thyroid hormones
Iodine ion (I-) is trapped through an aerobic process via active transport into the thyroid follicles. This starts the process of producing certain thyroid hormones
Injection of pertechnetate causes competitive inhibition of iodine concentration in the thyroid (99mTcO4- and I- compete for the available binding sites on the thyroid follicles)
Salivary glands, gastric mucosa, small intestine, mammary glands, skin, and hair trap iodine to a lesser degree (but it isn't organified)
Trapped iodine concentrations in the thyroid are between 25mg (normal) to as high as 5000mg (hyper) times that of the surrounding tissue