- Upper GI track bleeding usually caused by
- Gastric/duodenal ulcers
- Gastritis
- Varices (dilated or tortuous vein or artery)
- Lower GI track bleeding usually caused by (most GI bleeding procedure are seen as lower GI track bleeding)
- Diverticula
- Angiodysplasia (degenerative or congenital structural abnormality within the vascular structure of the GI track)
- Inflammatory bowel disease
- Neoplasm
- When blood leaks into the GI track significant irritation occurs resulting in a very rapid passing of bloody stool in forms of large purple clots (this usually occurs in the lower GI track)
- If a patient vomits blood (stomach) it appears as dark coffee grounds
- TMI?
- A high dose, usually between 10 to 15 mCi is administered, saturating the RES which allows for extended imaging within the GI track (normally a 5 mCi dose is cleared within minutes)
- In theory, the dose will extravasate out into the GI track and appear as a hot spot
- This will only occur is there is an active bleed
- Comments on the procedure
- Dynamic images can be taken for every 2 to 5 seconds for 1 minute
- Delayed images can be taken every 1 to 5 minutes at 500k per image
- The procedure is over when all activity has been engulfed by the RES how can you determine this?
- Comments on the use of sulfur colloid
- Sensitivity of this exam in dogs has shown the detection of a GI bleed with as little as 0.05 to 0.1 mL/minute this is twice as sensitive as a contrast angiogram
- As mentioned, if the patient has an intermittent bleed and is not bleeding at the time of the procedure, the bleed will not be detected
- Upper GI bleeds tend to be missed because of the excessive amount of activity in the liver
- Rectal hemorrhaging can also be missed and in theory, it is believed that attenuation from the pelvis may cause this (suggest that stool passed during the exam should be imaged to see if there is excessive activity in it)
- Consider the labeling procedure for this exam: in vivo, modified in vitro, and in vitro which one would have the least amount of background?
- Preferred is there is an intermittent bleed since imaging can be done for up to 24 hours
- However, the issue here is the need to catch the bleed as it first occurs
- Seeing the initial bleed allows for the identification or the specific location of the bleed endoscopy procedure can then be used to repair the bleed
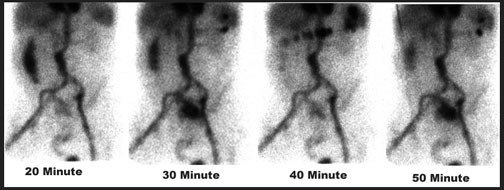
- If a pooling of blood is noted in a delayed image the question becomes exactly where did it occur
- Because of peristalsis or movement back and forth within the large bowel, it becomes difficult to excess the exact location of the bleed
- Consider an endoscopy procedure without knowing were the bleed is its like looking for a needle in a haystack
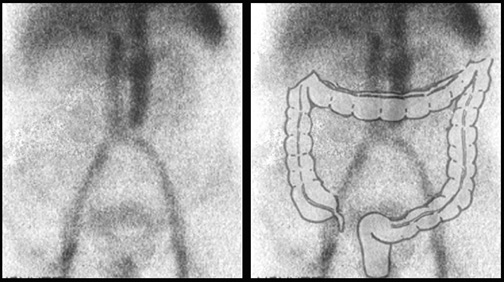
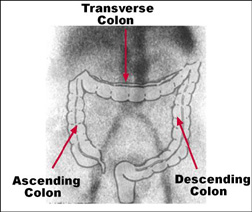
- Notice the above diagram where a negative GI bleeding image has an overlay of the GI track
- Ascending, transverse, and descending colon is identified
- A blush of activity occurring during imagine will define the location of the bleed
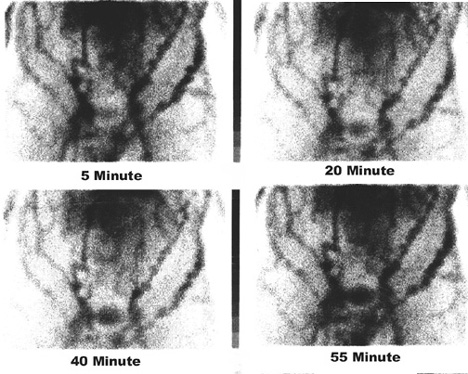
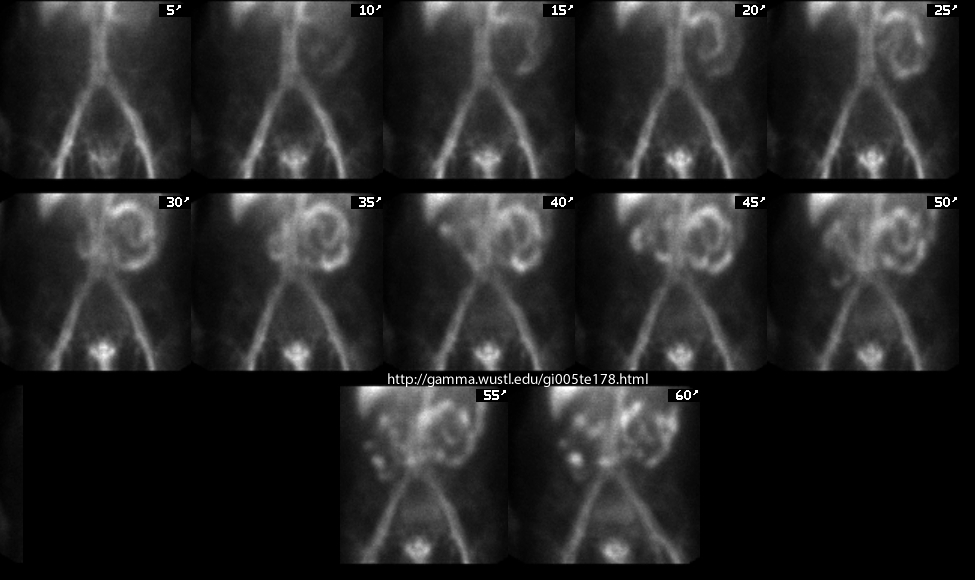
- A preferred method in imaging is to take 1 minute dynamic images for an hour following the injection of the labeled cells
- Additional 1 minute dynamics may be taken for an additional ½ to 1 hour pending the patients tolerance
- Delayed imaging can occur for up to 24 hours
- The longer it is between the injection and the delayed image the longer an image should be acquired consider the decay of technetium
- Optional imaging
- After your initial dynamic images (for 1 hour) take a static image over the thorax upper abdomen to assure that there is no bleeding within upper GI track
- However, bleeding in the upper GI track is usually noted in the lower GI track as the extravasated activity makes its way through the small bowel
- If youve injected the patient during the day and nothing abnormal is seen you might be called out in the middle of the night if rectal bleeding is noted
- After 24 hours, an additional dose of labeled red cells might be considered followed by another hour of imaging
- This would be done if rectal bleeding is noted, but the procedure looks negative
- At 24 hours post initial injection, extravasated blood will have significantly less activity and with a fresh dose of labeled RBCs the bleed may be more easily detected
- Sensitivity of RBCs requires approximately 3 mL of extravasated blood to be visualized (this may take up to 60 minutes to see in a slow bleed) were Sulfur Colloid requires 0.05 to 0.1 mL/minute
- RBCs can be imaged over a period of time (up to 24 hours)
- False positive RBC imaging can result from formation of free pertechnetate or unusual vascular structures why?
- RBC imaging is superior in imaging upper GI bleeding why?
- Studies have shown that sensitivity for GI bleeding is 12% with Sulfur Colloid and 93% with RBCs