99mTc Bio Routing
- What form is pertechnetate when eluted from the generator?
- In a an aqueous solution expressed in cations and anions and is written like this
- Na 99mTcO4-
 Na + + 99mTcO4-
Na + + 99mTcO4-
- Consider the oral administration of pertechnetate ...
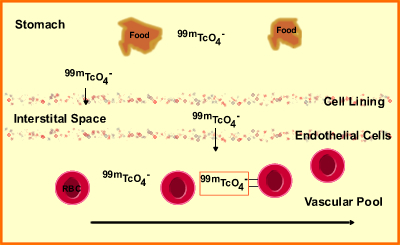
- From the diagram above 99mTcO4- is highly concentrated in the stomach cavity with no concentration beyond the cell lining of the stomach
- Therefore, it moves from into no concentrations areas as see above. This is referred to as _______________
- Pertechnetate passing through the cell lining of the stomach and reaches its first a fluid compartment known as interstitial space/fluid [IF] - note distribution throughout IF
- Then it passes the endothelial cells and enters the vascular compartment (VC)
- Gut content determines the rate of diffusion
- Fasting patient will have a maximum concentration of 99mTcO4-- in the blood within 30 minutes
- What happens when 99mTcO4- is administered IV?
- 100% of the dose immediately enters the blood stream
- Once in the VC, 99mTcO4- level begin to drop and is do to many physiological factors that will be discussed and you must define
- Physiologically
- 70 to 80% of the initial dose is partially bound to the RBC
- However, the porous nature of the endothelial lining allows passage of 99mTcO4-- out of the VC into the IF
- Molecular weight of less than 70,000 allows molecules to pass out of the VC into the IF
- Free 99mTcO4- has a molecular weight is 165 and passes into the IF
- Bound 99mTcO4- (RBC) initially stays in the VC because the molecular weight exceeds 70,000
- As the rate of free Tech drops, the partially bound 99mTcO4- breaks away from the RBC, becomes free, and then it might enter the IF
- In this process, 99mTcO4- pertechnetate continues to “seek” an equilibrium between the VC and IF (partially bound to RBC, free in the VC, and free in the IF)
- If you were to take a assess the VC and IF at “equilibrium” you would find that 75% of 99mTcO4- would be located in the IF. How can this be possible?
- Pertechnetate will also concentrate in the following organs: stomach, salivary glands, thyroid, bowel, mucous membranes, choroids plexus, brain, sweat glands and kidneys (Let’s take a look at these organs and how pertechnetate becomes physiologically involved
- Stomach
- In the stomach pertechnetate has a similarity to Cl- and replaces the CO2 in carbonic acid. Normally carbonic acid becomes hydrochloric acid
- Following IV administration 99mTcO4- reaches its highest concentration in the stomach
- Additionally, pertechnetate becomes reabsorbed into the stomach causing an internal cycle in its production
- It is the addition of other fluids that enter into the gut via swallowing fluids and gut secretions that force the pertechnetate into the small bowel. Also peristalsis aids in this process
- Small and large bowel
- Post 24 hr administration this area contains the highest concentration of pertechnetate
- As 99mTcO4- reaches maximum concentrations in the stomach, peristalsis, gut secretions and fluids taken PO, chyme (along with the pertechnetate) into the small bowel
- Secretion of fluids exceeds the absorbed volume making 99mTcO4- less likely to be reabsorbed
- In the large bowel chyme containing 99mTcO4- is trapped while the large bowel while excess fluid
- Bowel also extracts salts (this includes 99mTcO4-) into the its compartment via active transport through the cell membrane causing further concentration of these ion in the stool
- 30 to 40% 99mTcO4- is excreted
Questions - Can a 24-hour GI bleeding study using inVivo labeling identify blood in the stool?
- Salivary glands
- Saliva contains large amounts of salts similar to 99mTcO4- hence causing it to be extracted from the VC and IF
- There are four components in the salivary glands that cause visualization of pertechnetate
- Vascular
- Interstitial
- Cellular
- Secretion-collection
- It requires all four components to actually cause pertechnetate to be imaged in this area. Why?
- Saliva is isotonic, hence equal concentrates of salts are present inside and outside the gland
- If left only to this the salivary glands uptake of the ion would have reduced
- Maximum concentrations of activity occurs in 10 minutes
- Thyroid
- Why does it become trapped? But not organified?
- At 30 to 45 minutes pertechnetate reaches its maximum concentration
- Choroid Plexus
- You know this process – how does it cause increased uptake in the organ?
- What is the role of Lugol’s solution and KClO4-?
- Brain
- How does pertechnetate concentrate in this area? Or does it?
- When will you see a concentrated area of increased uptake?
- Kidneys
- Free pertechnetate enters the afferent arteriole and is removed
- Bound pertechnetate becomes unbound as it leaves the efferent arteriole
- Free pertechnetate moves into the VC from the IF
- Consider equal concentrations
- A process to remove free 99mTcO4- from the vascular pool
- 99mTcO4- levels must adjust after it leaves the kidneys
- Some of it is reabsorbed in the vascular pool in the tubules
- 50% of pertechnetate is excreted from the kidneys
- Can pertechnetate be used as a renal agent?
- Sweat glands
- Since pertechnetate is a salt it will be removed via the sweat glands
- Insensible perspiration – normal evaporation
- Sensible perspiration – where excess sweat to be produced and additional 99mTcO4- to be secreted
- Consider a patient in your department with sensible perspiration
Other thoughts
How would KClO4- affect pertechnetate uptake?
How does the body reduce its concentration of pertechnetate?
Why is the concentration of pertechnetate greater in the IF when compared to the VC?
Return to the Beginning of the Document
Return to the Table of Content
12/14