- Usually secondary to cirrhosis of the liver, the body fails to eliminate fluid from the peritoneal cavity. Therefore, fluid builds up. This is referred to as ascities. Under normal conditions the body produces and removes the fluid equally within this peritoneal cavity
- In order to relieve this build up of fluid a shunt is surgically implanted. It is referred to as a La Veen shunt
- The shunt runs from the peritoneal cavity to the jugular vein and then down to the superior vena cava
- A one-way valve allows for fluid to flow in the direction of the jugular vein
- When pressure in the peritoneum is greater than that of the superior vena cava, the fluid dumps into vascular pool
- The patient is also given specific breathing exercises to facilitate the pumping action
- A problem can arise when shunt becomes clogged. The cause might include
- Valve malfunction
- Thrombus
- Physiological problem with the patient: increased sodium levels, poor use of diuretics, or even liver/heart failure
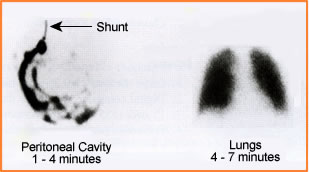
- Should this happen analysis of shunt function can be implemented with nuclear medicine
- Radiopharmaceutical - Usually, sulfur colloid or MAA, is administered intraperitoneally to determine if the shunt is still functioning. Post injection activity should exit the peritoneal cavity, dump into the vascular system and then the radiopharmaceutical is picked up by the liver/spleen or lungs, respectively. When this occurs shunt patency is defined. Failure for the organs to image means that there must be some type of blockage
- Procedure
- Setup
- Collimation - LEHR
- Window - 140 keV at 20%
- Acquire images at 500 to 1000k counts
- Setup sterile field for intraperitoneal injection
- Following the administration of a 3 mCi dose of MAA or sulfur colloid
- Image may occur ever 5 minutes for an hour or
- Dynamic images take be taken at 330 to 60 seconds per frame for an hour
- If the organ of interest does not shows up then delayed imaging should be done
- Suggested imaging for delays: 2 hours, 4 hours, end of the day, and first patient in the morning
- Setup
- Cases