There are three types of Leukocytes
-
Labeling with 111In oxine to the leukocyte
-
Labeling Leukocyte Procedure
-
Labeling efficiency is difficult to determine
-
Pathophysiology of 111In-WBC
-
111In-WBC Procedure
- Comments on 99mTcWBC imaging

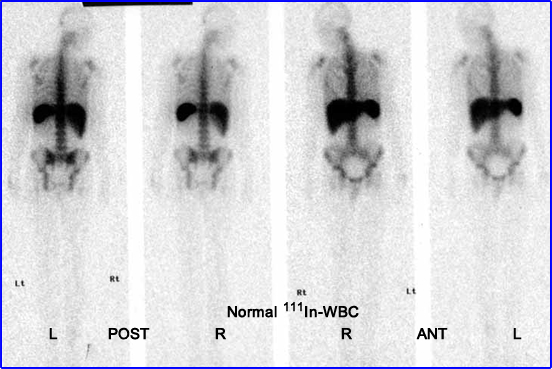
- Above is a side by side exam of what a normal Gallium Scan and normal 111In-WBC scan

- Here is another example that shows Indium labeled with 99mTc with 4 and 24 hours.1What is the difference? Consider physiology. Consider count density.
- Granulocytes
- Lymphocytes
- Monocytes
- Oxine is a lipohilic ligand that chelates to certain metals, which includes In
- 111In oxine is lipid soluble and diffuses through red and white blood cells
- Once inside 111In binds to the cell and oxine is released and can be separated from solution
- The amount of tagged WBCs depends on the amount of WBCs in solution
- Question - If 1.0 mCi of 111In oxine is added to tag the WBCs and only 0.4 mCi of tagged WBCs is returned, does that mean that there is only a 40% tag?
- No, there was only enough WBCs present to tag 0.4 mCi with 111In oxine. The remainder indium is removed when the cells are washed with the PPP
- From the mix of tagged leukocytes the WBCs will accumulate at sites of infection
- Following the 111In-WBC injection activity can be seen the lungs, liver, spleen, and blood pool
- Over several hours lung activity will decrease
- At 18-24 hours normal concentration of activity is seen in the liver, spleen, and bone marrow
- Activity seen greater than the liver is considered an infectious site
- Activity equal to or less than or equal to the liver maybe an inflammatory process
- Activity less than bone marrow is probably not an infection
- Unlike 67Ga, labeled WBCs will not be seen in the urinary track, bowel, or colon
- In chronic infection, WBC may be unable to penetrate the infection which may be do to lack of circulation or the infection may be "walled off." Hence 67Ga is preferred
- Following the injection of the radiotracer imaging should be done between 18-24 hours post dose
- Whole body set-up - generally starting at the head and ending at mid-thigh
- Energy settings
- 173 keV at 20%
- 247 keV at 20%
- Collimator - ME
- Whole body format
- Head to mid-thigh (unless disease is present in the appendages)
- Scan speed of 10 cm/minute or less
- 256 x 1024 matrix or greater
- Spot imaging
- Matrix - 256
- 15 minutes per image
- When 99mTcHMPAO is mixed with the WBCs the complex becomes hydrophilic causing the tracer to become trapped within the cell (WBC). The tracer binds to the intracellular organelles, mostly in the mitochondria and nucleus
- Distribution of the radiotracer is seen in spleen, liver, and bone marrow. However, activity is also seen in the kidneys, bladder, and bowel (do to GB excretion). Activity is also seen in the lung for up to four hours post dose
- Comparing 111In tag to 99mTc tag
- Literature review indicates that 99mTcWBC is superior to 111InWBC. A study was done where both agents at the same time and dual isotope imaging was performed
- Imaging with the 99mTc agent can be done as early as 30 minutes to 1 hour
- Sensitivity is between 92 and 100% (which is better than 111InWBC)
- Excretion of the 99mTc product may result in some difficulty when imaging the lower abdominal area since the product is excreted though the bowel and kidneys, especially if delayed imaging is done at 4 hours post dose. Imaging at 1 hour post dose elevates the this problem when imaging the bowel
Return to the Beginning of the Document
Return to the Table of Content
Leukocyte Imaging Procedures (In-111 and Tc99m)
8/14
Reference
1- Radionuclide Imaging of Infection by Love, C, et al.