- Metal implants
- Motion artifacts
- Oral and venous contrast
- Truncation
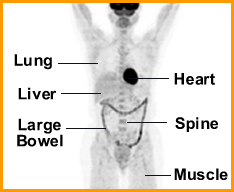
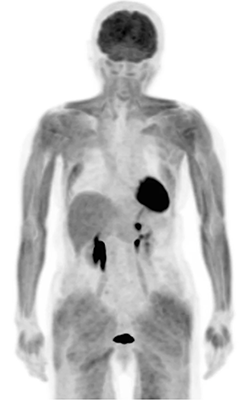
- Heart
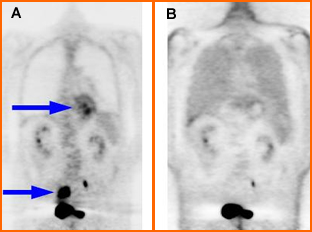
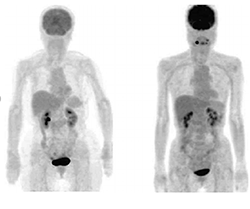
- Uptake of FDG depends on the patient's glucose level
- At low glucose levels the heart metabolic mechanism requires fatty acids, which is its preferred method for using its energy
- Given the above two images one has a glucose level of 221 and the other of 100 mg/dL. Which is which?
- If the glucose level is low and if FDG is injected, uptake by the myocardium will be insignificant
- After eating, the glucose level increases and the heart's switches is metabolic need to glucose
- Therefore, patients scheduled for a PET scan are required to be NPO, because this will result in reduces FDG uptake in the myocardium. Literature indicates that fasting reduces cardiac uptake in 80% of the patient population
- If the patient has a high glucose levels (above 200) FDG injection becomes more competitive and reduced radio-tracer uptake will occur
- Uptake of FDG occurs as follows if the sugar level is a normal range (<200 mg/dL)
- 0 - 20 minutes most of the activity is found in the vascular pool (heart ventricles)
- 20 - 60 minutes (over time) activity leaves the vascular pool and perfuses slowly into myocardial tissue
Link to Research Paper - Arterial
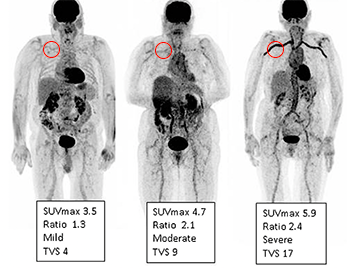
- There may be some (mild) activity in the aorta's thoracic region which is considered normal
- Increased muscle tone, inflammation, or arterial plaque (containing WBCs) may show increased uptake in the related areas
- While glucose is reabsorbed by the kidneys, FDG is not, hence there is significant activity in the kidneys and urinary bladder
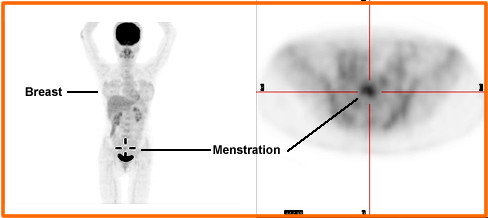
- Urine contamination may be seen as hot spots on the surface of the skin or in the general area of the groin
- Tampon uptake is noted. This was caused by urine contamination
- If a contrast agent is administered prior to a PET scan, contrast in the bladder and/or kidneys will generate artifacts on the attenuated PET scan
- To reduce urinary bladder activity have the patient void prior to imaging. It is also suggested that you start the scan at the feet/thigh to reduce urinary filling of the bladder
- If the pelvic region is the area of concern a Foley catheter may be considered

http://www.springerlink.com/content/53um5n17240875h7/
- There can be varying degrees of uptake with little to intense activity within the bowel
- Activity is usually the greatest in the large bowel
- Currently there is no method to reduce FDG uptake in the GI region
- Reflux, radiation therapy, or inflammation of the esophagus may cause FDG uptake
- Stomach may be seen and is probably related to peristalsis (remember muscle movement)
- Intestinal uptake can be seen and may relate to: peristalsis, WBC concentration, or secretion of FDG into GI track
- Normal liver uptake is possible and is more prevalent in the unattenuated PET imagines. Hepatocytes do not excrete FDG
- Spleen has little to no uptake. Likewise the pancreas should not visualize
- Respiration/liver artifact (motion defect) can be noted in the area around the dome of the liver. This is caused by motion and attenuation correction
- Diverticulitis will show "beads" of activity on the intestinal track which indicate areas of infection
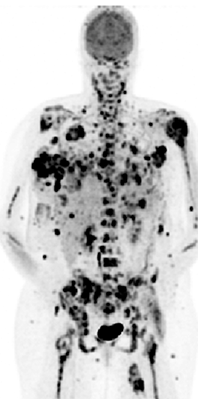
- Bone marrow
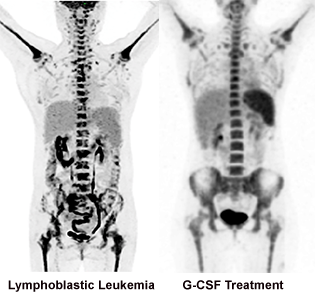
https://www.researchgate.net/- Activated marrow is visualized (more in the central skeleton) with FDG which is due to FDG accumulation in WBCs and RBCs production
- Single or multiple foci may indicate metastatic disease in the marrow
- Chemotherapy will activate bone marrow production
- Lymph node uptake indicates disease
- From the above image can you tell the difference between lymphoblastic leukemia and granulocyte colony stimulating factor (G-CSF)
- Thymus may appear as a V shaped object and is considered normal. The above thymus is enlarged representing thymic hyperplasia after therapy
- Thyroid uptake may also be noted, however, asymmetry is an indication of disease
- Parathyroid can have moderate uptake and still be considered normal
- Muscles uptake in the neck occurs when the patient is talking or moving there head post FDG administration
- Little to no uptake is seen in the: adrenals, ovaries, or testicular

http://www.scielo.br/scielo.php?pid=S1516-84842011000200013&script=sci_arttext
- There should be little to no uptake in bone
- Note bone marrow uptake can be the reason for "bone uptake"
- Too much free 18F will cause increased uptake in the bony matrix
- CT corrected PET images in the presence of metal will cause falsely elevated uptake levels in the bone
- Joint uptake can be see as normal even with a moderate level of activity. Joint activity usually increases with age and is most common in the acromioclavicular area. This can be an area of chronic inflammation
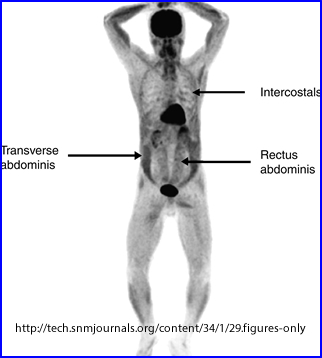
- Muscle uptake can be seen for various reason
- Exercise of muscles just prior, during, and/or up to 1 hour post FDG administration
- If the patient has not fasted for 4 hours prior to his/her injection
- Patients will elevated blood sugar forces FDG uptake to muscle
- Diabetics with high glucose levels
- Talking, eye movement, hiccups may cause muscle uptake in the related areas
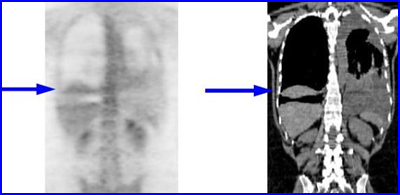
- The above image is of a patient with a chronic cough and post FDG administration
- In a similar analysis this patient was only NPO for 2 hours resulting in excessive muscle uptake
Link to reference
- There may be some mild uptake in the attenuation corrected images
of the skin
- Activity on the skin is due to the lack of attenuation at the surface of body therefore increased amount of counts on acquisition
- CT attenuation tends to correct this anomaly
- Increased skin uptake may hide pathology related certain skin cancers
https://www.researchgate.net/ - Little to no activity is seen in the connective tissue
- If activity is seen it is probably related to muscular uptake
- Implants may cause PET artifacts with CT correction
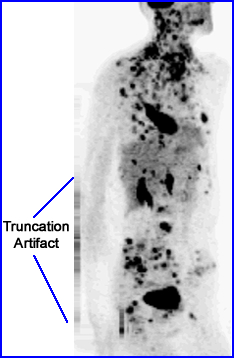
- CT corrected PET images have shown striped artifacts in the area of the edge of the CT's FOV and relate to truncation. Remember that the FOV of PET is larger and this artifact is generated where the FOV of CT ends and the PET FOV continues. Bariatric patients will by nature have a greater amount of these defects
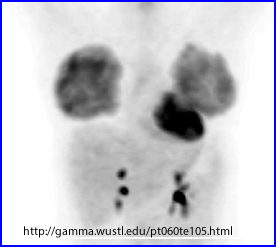
- Breast activity can be noted for several reasons
- Specifically in patients that are in the later phase of menstruation
- FDG is secreted during lactation which will show up as very intense uptake at the site, as in the case in the above image
-
Breast implants may show activity along the edge. This is do to a chronic inflammatory reaction. Did not find a patient with chronic infection, however, there were numerous cases with disease: Case 1 and Case 2. Would you be able to tell the difference between infection and cancerous disease?and
- SUV = measured activity/voxel x Patient weight/injected activity
- The more involved formula is noted above
- What do you need to do to really make this work?
- Get the exact weight of the patient
- Determine the exact amount of activity injected into the patient (subtract post syringe counts)
- Attempt to administer the same amount of activity on return visits
- Always image at the same time post injection (very important when comparing previous studies)
- Calibrate all the clocks in the department to the same time
- Scanner must be calibrated correctly